En el cuerpo humano, encontramos algunas lesiones en las que el tejido lesionado, cuanto más dañado esté, más se potencia el mecanismo lesivo, conllevando un mayor daño, lo que favorece aún más el mecanismo lesivo, que agrava el daño….. y así sucesivamente hasta el infinito, como círculo vicioso, como pescadilla que se muerde la cola. Y resulta que el Síndrome del trocánter mayor es una de esas lesiones.
En la primera entrega de esta trilogía («La Epidemia de la cadera: Síndorme del trocánter mayor«) nos centramos en presentar este síndrome, en este segundo queremos explicar el mecanismo lesivo, y en la tercera haremos la propuesta de trabajo.
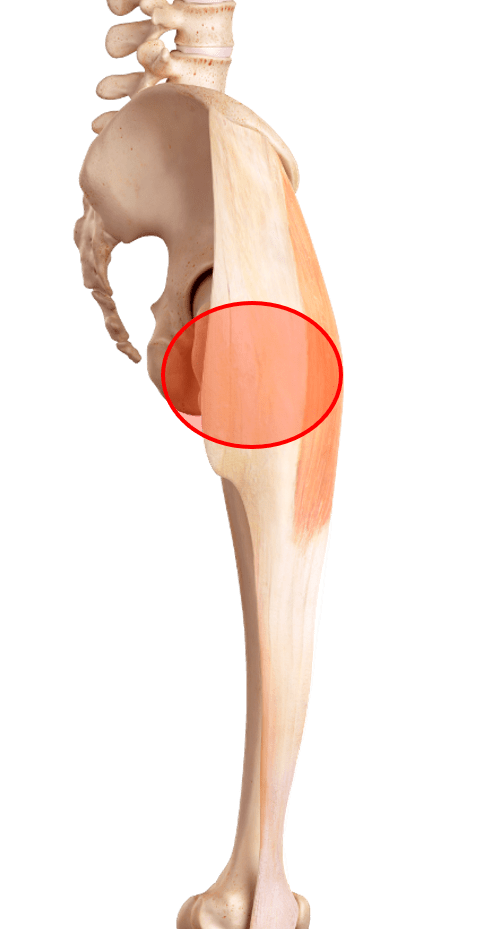
Síndrome trocánter mayor
Mecanismo lesivo:
Como en cualquier tendinopatía o burstis, el sobreuso suele ser la causa principal, pero como en cualquier afectación, el problema es multifactorial, y habrán a menudo factores biomecánicos que van a contribuir a que exista un mayor estrés en determinados tejidos, como la Coxa Saltans externa o el impingement externo.
Coxa Saltans externa:
Hace referencia a los “chasquidos que se pueden escuchar o sentir en el lateral de la cadera, al pasar la parte posterior de la cintilla iliotibial o porción anterior del tendón del glúteo mayor, a un lado y otro del trocánter mayor. Esta puede ser una causa del síndrome del trocánter mayor, pero se ha comprobado que muchas personas que presentan esta condición no desarrollan el síndrome74.
Impingement Externo:
La cintilla iliotibial puede causar impingement externo sobre el trocánter mayor, ya que provoca irritación por compresión de los tendones glúteos12,24,33,37, lo que se aumenta con la aducción de cadera y la inclinación pélvica contralateral9. Por ello en la fase aguda se debe evitar excesiva tensión sobre el glúteo mayor y el tensor de la fascia lata; igualmente evitar el masaje con foam roller en la fase aguda por añadir mayor carga por compresión.
Los corredores que aducen la cadera provocando apoyos más allá de la línea media durante el ciclo de la marcha, tienen más posibilidades de sufrir este síndrome18. Lo cual puede ser explicado porque las cargas compresivas son dependientes de la posición, siendo de 4N a 0º, 36N a 10º de aducción, y 106N a 40º de aducción9. Por ello, se ha relacionado con el mantenimiento de posturas como las piernas cruzadas.
Grimaldi et al presenta un cuadro muy interesante sobre la respuesta biológica de los tendones ante diferentes tipos de carga:

La compresión y la privación de cargas por tensión inducen a la aparición de enzimas catabólicas a nivel celular, lo que produce rotura del colágeno Tipo169.
La compresión transversal en este síndrome se produce por el mecanismo que llamábamos impingement externo.
¿Pero porqué decimos que esta lesión es como una pescadilla que se muerde la cola?
La fuerza de abducción envuelve dos sinergias musculares9,34,35,70
- Los Músculos trocantéreos: Glúteo medio y glúteo menor.
- Los Músculos tensores de la Cintilla Iliotibial: Porción superior del glúteo mayor, El tensor de la Fascia Lata y el Vasto externo del cuádriceps.

Se ha calculado que el 70% de la Fuerza abductora requerida en un apoyo monopodal lo ejercen los músculos trocantéreos, mientras que el 30% a los músculos tensores de La Cintilla Iliotibial. La relación TFL-GMedio se puede ver alterada con frecuencia produciendo una dominancia del TFL sobre el GMedio en la abducción de cadera, lo que suele guiar a debilidad y/o atrofia del GMedio11,29,59. Se ha demostrado que las personas que sufren desgarros de los tendones glúteos trocantéreos tienen hipertrofia ipsilateral del tensor de la fascia lata68.
El desequilibrio entre estas dos sinergias musculares va a estar detrás de los tres mecanismos lesivos expuestos anteriormente: Sobreuso, coxa saltans, impingement externo. Por lo que la debilidad de los músculos trocantéreos y la tensión de los músculos tensores de la cintilla iliotibial se puede convertir en un peligroso círculo vicioso. Conforme más debilidad de los glúteos, mayor sobreuso de los tensores de la cintilla que se transformará en mayor tensión de este complejo, favoreciendo el impingement externo y/o la coxa saltans, pudiendo dañar los tendones del glúteo medio y menor, lo que implica mayor debilidad aún, y vuelta a empezar con el círculo vicioso.
FACTORES:
- Ratio TFL/GMP (Tensor de la fascia lata/Glúteo medio posterior).
- Tener un índice de masa corporal superior a la media28
- Adiposidad elevada31
- Morfología de la pelvis femenina10,30,57,63, lo que podría explicarse por la pelvis más amplia, que implica diferencias biomecánicas48, aunque también se ha especulado que puede influir que la inserción del tendón del glúteo medio tiene un área menor, por lo que tiene menor capacidad de disipación de las fuerzas, además de tener un menor brazo de momento, lo que resulta en una reducida eficiencia mecánica77.
Ya hemos entendido los mecanismos que producen este síndrome, así que ya estamos en disposición de buscar la solución. Es bastante evidente, pero para saber cómo planteamos nosotros el trabajo, a leerse la tercera parte de esta trilogía. ¡Síndrome del trocánter mayor!, ¡Prepárate! tenemos la vacuna para tu epidemia.

Preguntas frecuentes sobre el síndrome trocánter mayor
¿Qué es síndrome doloroso del trocánter mayor?
El síndrome doloroso del trocánter mayor, también conocido como trocanteritis o bursitis trocantérea, es una condición dolorosa que afecta la región lateral de la cadera. Esta área se encuentra en la parte superior del fémur, en la zona denominada trocánter mayor.
El síndrome doloroso del trocánter mayor se caracteriza por dolor y sensibilidad en el área del trocánter mayor, que puede extenderse hacia el muslo o la parte externa de la pierna. Algunos de los síntomas comunes incluyen:
- Dolor en la cadera: El dolor suele ser localizado en la parte lateral de la cadera, en la región del trocánter mayor. Puede ser constante o aparecer al realizar actividades como caminar, subir escaleras o levantarse de una silla.
- Sensibilidad al tacto: La zona afectada puede ser sensible al tacto, lo que significa que puede haber dolor al presionar o palpar el área del trocánter mayor.
- Dolor al estar acostado de lado: Muchas personas experimentan un aumento del dolor al estar acostadas de lado en la cama, ya que se ejerce presión directa sobre el trocánter mayor.
- Limitación en los movimientos: En algunos casos, el síndrome del trocánter mayor puede causar dificultad para mover la cadera o realizar actividades que implican la rotación o abducción de la pierna.
Las causas del síndrome doloroso del trocánter mayor pueden variar e incluir la inflamación de la bursa trocantérea (bursitis), lesiones en los tendones que rodean el trocánter mayor (tendinitis), irritación de los músculos de la cadera o la fricción excesiva entre los tejidos.
El tratamiento del síndrome doloroso del trocánter mayor generalmente incluye medidas conservadoras, como el reposo, la aplicación de hielo, el uso de medicamentos antiinflamatorios, la fisioterapia, los ejercicios de fortalecimiento y estiramientos específicos, así como la corrección de posibles desequilibrios musculares o problemas biomecánicos.
Si experimentas dolor en la región lateral de la cadera o sospechas de síndrome doloroso del trocánter mayor, es recomendable buscar atención médica para obtener un diagnóstico preciso y un plan de tratamiento adecuado
¿Cómo se cura una trocanteritis de cadera?
El tratamiento de la trocanteritis de cadera, también conocida como síndrome doloroso del trocánter mayor, se basa en enfoques conservadores para aliviar el dolor y promover la curación. A continuación, se describen algunas medidas comunes utilizadas en el tratamiento de esta condición:
- Reposo y modificación de actividades: Es importante reducir o evitar las actividades que puedan agravar el dolor, como correr, saltar o subir escaleras. El reposo relativo puede ayudar a reducir la inflamación y permitir que los tejidos se recuperen.
- Aplicación de hielo: Aplicar hielo en el área afectada puede ayudar a reducir la inflamación y aliviar el dolor. Se recomienda aplicar hielo durante 15-20 minutos varias veces al día, evitando aplicarlo directamente sobre la piel y utilizando una barrera protectora, como una toalla.
- Medicamentos antiinflamatorios: Los medicamentos antiinflamatorios no esteroides (AINE), como el ibuprofeno o el naproxeno, pueden ayudar a reducir la inflamación y aliviar el dolor. Sin embargo, es importante seguir las indicaciones del médico y respetar las dosis recomendadas.
- Fisioterapia: Un fisioterapeuta puede desempeñar un papel importante en el tratamiento de la trocanteritis de cadera. Los ejercicios de fortalecimiento y estiramiento específicos pueden ayudar a mejorar la estabilidad de la cadera, reducir la tensión en los músculos y tendones afectados, y promover una mejor biomecánica de la cadera.
- Terapia de ondas de choque: En algunos casos, se puede considerar la terapia de ondas de choque como una opción de tratamiento. Este enfoque utiliza ondas de sonido de alta energía para estimular la curación de los tejidos y reducir la inflamación.
- Uso de dispositivos de apoyo: Dependiendo de la situación, se pueden utilizar dispositivos de apoyo, como férulas, almohadillas o calzado ortopédico, para reducir la carga y la presión sobre el área afectada y mejorar la función de la cadera.
¿Qué no debo hacer si tengo trocanteritis?
- Evita actividades que aumenten el dolor: Evita realizar actividades que provoquen un aumento significativo del dolor en la región del trocánter mayor. Esto puede incluir correr, saltar, subir escaleras o cualquier movimiento que cause molestias intensas.
- No ignores el dolor persistente: No ignores el dolor persistente en la cadera o en el área del trocánter mayor. Ignorar los síntomas y continuar con actividades que agravan el dolor puede empeorar la condición y prolongar la recuperación.
- Evita la falta de movimiento: Si bien es importante descansar y evitar actividades que provoquen dolor, también es esencial mantener cierto nivel de movimiento y movilidad en la cadera. La inmovilidad prolongada puede llevar a la rigidez y debilidad muscular. Realiza movimientos suaves y controlados dentro de los límites de dolor, según lo recomendado por un profesional de la salud.
- No te automediques sin supervisión médica: Evita automedicarte sin la supervisión de un profesional de la salud. Si bien los medicamentos antiinflamatorios pueden ser útiles para aliviar el dolor y reducir la inflamación, es importante seguir las indicaciones médicas y respetar las dosis recomendadas.
- No ignores la importancia de la fisioterapia: La fisioterapia puede desempeñar un papel crucial en el tratamiento de la trocanteritis. No ignores la importancia de seguir las pautas y recomendaciones de tu fisioterapeuta, incluyendo los ejercicios de fortalecimiento, estiramientos y técnicas de terapia manual.
- Evita el exceso de actividad física: Evita realizar ejercicio físico intenso o prolongado que pueda sobrecargar la cadera y los músculos de la zona. El exceso de actividad puede aumentar la irritación y prolongar el tiempo de recuperación.
¿Cómo se quita el dolor de la trocanteritis?
La trocanteritis, también conocida como tendinitis de la cadera o dolor en el trocánter mayor, puede ser muy incómoda y dolorosa. Aquí tienes algunas recomendaciones para ayudar a aliviar el dolor de la trocanteritis:
- Reposo: Descansa la cadera afectada y evita actividades que puedan empeorar el dolor, como correr, saltar o levantar objetos pesados. Descansar la articulación inflamada puede permitir que se recupere más rápido.
- Aplicación de hielo: Aplicar hielo en la zona dolorida durante 15-20 minutos varias veces al día puede reducir la inflamación y aliviar el dolor. Asegúrate de envolver el hielo en una toalla o paño para evitar quemaduras en la piel.
- Antiinflamatorios no esteroides (AINEs): Los medicamentos de venta libre, como el ibuprofeno o el naproxeno, pueden ayudar a reducir el dolor y la inflamación. Sigue las indicaciones del envase o consulta a un profesional de la salud antes de tomar cualquier medicamento.
- Fisioterapia: Un fisioterapeuta puede diseñar un programa de ejercicios específicos para fortalecer los músculos alrededor de la cadera y mejorar la movilidad. Esto puede ayudar a aliviar la presión sobre la articulación y reducir el dolor a largo plazo.
- Estiramientos y ejercicios de movilidad: Realizar ejercicios suaves de estiramiento y movilidad puede ayudar a mantener la flexibilidad y prevenir la rigidez en la cadera. Un fisioterapeuta puede enseñarte ejercicios adecuados.
- Corrección de la postura y ergonomía: Asegúrate de mantener una postura adecuada al estar de pie o sentado, y utiliza una silla con un buen soporte lumbar si trabajas en un escritorio durante largos períodos.
- Cambios en la actividad física: Si el dolor es causado por actividades específicas, como correr o caminar en superficies duras, considera hacer cambios en tu rutina de ejercicios o utilizar calzado adecuado.
- Terapia de ondas de choque: En algunos casos, la terapia de ondas de choque extracorporales puede ser recomendada por un profesional de la salud para estimular la curación y reducir la inflamación en la zona afectada.
- Inyecciones de corticosteroides: En casos graves, un médico puede recomendar inyecciones de corticosteroides en la articulación para reducir la inflamación y el dolor. Este procedimiento debe ser realizado por un profesional de la salud.
Es importante recordar que el tratamiento de la trocanteritis puede variar según la causa subyacente y la gravedad del dolor. Es recomendable consultar a un médico o fisioterapeuta para un diagnóstico adecuado y un plan de tratamiento personalizado. No intentes autodiagnosticar ni automedicarte sin consultar a un profesional de la salud.
¿Qué es mejor para la trocanteritis el frío o el calor?
Tanto el frío como el calor pueden ser útiles en el manejo de la trocanteritis, pero su aplicación depende de la etapa y la sensación individual de alivio que proporcionen. Aquí te explico cuándo es más adecuado utilizar cada uno:
Frío (aplicación de hielo):
- Fase aguda de la lesión: Cuando experimentas un aumento reciente en el dolor o inflamación debido a la trocanteritis, la aplicación de hielo puede ser beneficiosa. El frío ayuda a reducir la inflamación y alivia el dolor al disminuir la actividad de los nervios en la zona.
- Dolor agudo o después de la actividad: Aplicar hielo después de realizar actividades que desencadenen dolor o después de realizar ejercicios de rehabilitación puede ayudar a reducir la inflamación y aliviar el malestar.
- Cómo aplicar: Envuelve el hielo en una toalla o paño para evitar quemaduras en la piel y aplícalo en la zona afectada durante 15-20 minutos a la vez, varias veces al día según sea necesario.
Calor:
- Fase de recuperación y relajación muscular: Una vez que la inflamación inicial ha disminuido y el dolor agudo ha cedido, el calor puede ser útil para relajar los músculos circundantes y aumentar el flujo sanguíneo. Esto puede ayudar en la recuperación a largo plazo.
- Antes de ejercicios de estiramiento o rehabilitación: Aplicar calor antes de realizar ejercicios de estiramiento o movilidad puede ayudar a aumentar la flexibilidad y reducir el riesgo de lesiones musculares.
- Cómo aplicar: Puedes utilizar una almohadilla térmica, una compresa caliente o incluso un baño caliente. Asegúrate de no aplicar calor directamente sobre la piel y evita temperaturas excesivamente altas.
BIBLIOGRAFÍA:
-
Allison K, Bennell KL, Grimaldi A, Vicenzino B, Wrigley TV, Hodges PW. Single leg stance control in individuals with symptomatic gluteal tendinopathy. Gait Posture. 2016 Sep;49:108-13.
-
Allison K, Vicenzino B, Wrigley TV, Grimaldi A, Hodges PW, Bennell KL. Hip Abductor Muscle Weakness in Individuals with Gluteal Tendinopathy. Med Sci Sports Exerc. 2016 Mar;48(3):346-52.
-
Allison K, Wrigley TV, Vicenzino B, Bennell KL, Grimaldi A, Hodges PW. Kinematics and kinetics during walking in individuals with gluteal tendinopathy. Clin Biomech (Bristol, Avon). 2016 Feb;32:56-63.
-
Bancroft LW, Blankenbaker DG. Imaging of the tendons about the pelvis. AJR Am J Roentgenol. 2010;195:605-617.
-
Barnthouse NC, Wente TM, Voos JE. Greater trochanteric pain syndrome: endoscopic treatment options. Oper Tech Sports Med. 2012;20:320–324.
-
Berry JW, Lee TS, Foley HD, Lewis CL. Resisted Side Stepping: The Effect of Posture on Hip Abductor Muscle Activation. J Orthop Sports Phys Ther. 2015 Sep;45(9):675-82.
-
Bewyer DC, Bewyer KJ. Rationale for treatment of hip abductor pain syndrome. The Iowa Orthopaedic Journal. 2003;23:57-60.
-
Bird PA, Oakley SP, Shnier R, Kirkham BW. Prospective evaluation of magnetic resonance imaging and physical examination findings in patients with greater trochanteric pain syndrome. Arthritis Rheum. 2001 Sep;44(9):2138-45.
-
Birnbaum K, Siebert CH, Pandorf T, Schopphoff E, Prescher A, Niethard FU. Anatomical and biomechanical investigations of the iliotibial tract. Surgical and Radiologic Anatomy. 2004;26:433-46.
-
Blank E, Owens BD, Burks R, Belmont PJ Jr. Incidence of greater trochanteric pain syndrome in active duty US military service members. Orthopedics. 2012 Jul 1;35(7):e1022-7.
-
Brody, LT.; Hall, CM. Therapeutic exercise: Moving toward function. 3rd. Lippincott Williams & Wilkins; Baltimore: 2011.
-
Bunker TD, Esler CNA, Leach WJ. Rotator-Cuff Tear of the Hip. Journal of Bone & Joint Surgery – British Volume. 1997;79-B(4):618-20.
-
Cambridge ED, Sidorkewicz N, Ikeda DM, McGill SM. Progressive hip rehabilitation: The effects of resistance band placement on gluteal activation during two common exercises. Clin Biomech (Bristol, Avon). 2012; 27(7):719–24.
-
Chandrasekaran S, Vemula SP, Gui C, Suarez-Ahedo C, Lodhia P, Domb BG. Clinical Features That Predict the Need for Operative Intervention in Gluteus Medius Tears. Orthopaedic Journal of Sports Medicine. 2015;3(2):2325967115571079. doi:10.1177/2325967115571079.
-
Chi AS, Long SS, Zoga AC, Read PJ, Deely DM, Parker L, Morrison WB. Prevalence and pattern of gluteus medius and minimus endon pathology and muscle atrophy in older individuals using MRI. Skeletal Radiol. 2015 Dec;44(12):1727-33.
-
Chowdhury R, Naaseri S, Lee J, Rajeswaran G. Imaging and management of greater trochanteric pain syndrome. Postgrad Med J. 2014 Oct;90(1068):576-81.
-
Chumanov ES, Wille CM, Michalski MP, et al. Changes in muscle activation patterns when running step rate is increased. Gait Posture. 2012;36(2):231–5.
-
Clancy WG. Runners’ injuries: part two. Evaluation and treatment of specific injuries. Am J Sports Med. 1980;8(4):287–9.
-
Collee G. Greater trochanteric pain syndrome (trochanteric bursitis) in low back pain. Scand J Rheumatol. 1991;20:262–266
-
Cook JL, Purdam C. Is compressive load a factor in the development of tendinopathy? Br J Sports Med. 2012;46:163-168.
-
Cook JL, Purdam CR. The challenge of managing tendinopathy in competing athletes. Br J Sports Med. 2014;48:506-509.
-
Cook JL. Is tendon pathology a continuum? A pathology model to explain the clinical presentation of load-induced tendinopathy. British Journal of Sports Medicine. 2009;43(6):409-16.
-
Del Buono A, Papalia R, Khanduja V, et al. Management of the greater trochanteric pain syndrome: a systematic review. Br Med Bull. 2012;102:115–31.
-
Dwek J, Pfirrmann C, Stanley A, Pathria M, Chung CB. MR imaging of the hip abductors: normal anatomy and commonly encountered pathology at the greater trochanter. Magnetic Resonance Imaging Clinics Of North America. 2005;13(4):691.
-
Ebert JR, Retheesh T, Mutreja R, Janes GC. THE CLINICAL, FUNCTIONAL AND BIOMECHANICAL PRESENTATION OF PATIENTS WITH SYMPTOMATIC HIP ABDUCTOR TENDON TEARS. International Journal of Sports Physical Therapy. 2016;11(5):725-737.
-
Ege Rasmussen KJ, Fanø N. Trochanteric bursitis. Treatment by corticosteroid injection. Scand J Rheumatol. 1985;14(4):417-20.
-
Fearon AM, Cook JL, Scarvell JM, Neeman T, Cormick W, Smith PN. Greater Trochanteric Pain Syndrome Negatively Affects Work, Physical Activity and Quality of Life: A Case Control Study. J Arthroplasty. 2014;29(2):383-6.
-
Fearon AM, Stephens S, Cook JL, Smith PN, Cormick W, Scarvell JM. Are child bearing hips a risk factor for greater trochanteric pain syndrome? J Bodyw Mov Ther. 2012;16:148.
-
Fredericson M, Cookingham CL, Chaudhari AM, Dowdell BC, Oestreicher N, Sahrmann SA. Hip abductor weakness in distance runners with iliotibial band syndrome. Clin J Sport Med. 2000; 10(3):169–75
-
Furia JP, Rompe JD, Maffulli N. Low-energy extracorporeal shock wave therapy as a treatment for greater trochanteric pain syndrome. The American journal of sports medicine. 2009;37(9):1806- 1813.
-
Gaida JE, Ashe MC, Bass SL, Cook JL. Is adiposity an underrecognized risk factor for tendinopathy? A systematic review. Arthritis Rheum. 2009;61(6):840–9.
-
Grimaldi A, Fearon A. Gluteal Tendinopathy: Integrating Pathomechanics and Clinical Features in Its Management. J Orthop Sports Phys Ther 2015;45(11):910-922.
-
Grimaldi A, Mellor R, Hodges P, Bennell K, Wajswelner H, Vicenzino B. Gluteal Tendinopathy: A Review of Mechanisms, Assessment and Management. Sports Med. 2015;48(8):1107-19.
-
Grimaldi A. Assessing lateral stability of the hip and pelvis. Manual Therapy. 2011;16:26-32.
-
Grimaldi A, Richardson C, Stanton W, et al. The association between degenerative hip joint pathology and size of the gluteus medius, gluteus minimus and piriformis muscles. Man Ther. 2009;14(6):605–10.
-
Heiderscheit BC. Lower extremity injuries: is it just about hip strength? J Orthop Sports Phys Ther. 2010;40(2):39–41.
-
Ho GW, Howard TM. Greater trochanteric pain syndrome: more than bursitis and iliotibial traction friction. Curr Sports Med Rep. 2012 Sep-Oct;11(5):232-8.
-
Huang BK, Campos JC, Michael Peschka PG, Pretterklieber ML, Skaf AY, Chung CB, Pathria MN. Injury of the gluteal aponeurotic fascia and proximal iliotibial band: anatomy, pathologic conditions, and MR imaging. Radiographics. 2013 Sep-Oct;33(5):1437-52.
-
Iorio R, Healy WL, Warren PD, Appleby D. Lateral trochanteric pain following primary total hip arthroplasty. J Arthroplasty. 2006;21:233-236.
-
Kagan II A. Rotator cuff tears of the hip. Clin Orthop. 1999;368: 135–40.
-
Kagan II A. Rotator-cuff tear of the hip. J Bone Joint Surg (Br). 1998;80(1):182–3.
-
Kaltenborn A, Bourg CM, Gutzeit A, Kalberer F. The Hip Lag Sign – Prospective Blinded Trial of a New Clinical Sign to Predict Hip Abductor Damage. PLoS One. 2014; 9(3): e91560.
-
Ker RF, Wang XT, Pike AV. Fatigue quality of mammalian tendons. The Journal of experimental biology. 2000;203(Pt 8):1317-27.
-
Kimpel DM, Garner CC, Magone KM, May JH, Lawless MW. Greater trochanteric hip 583 pain. Orthop Nurs. 2014 Mar-Apr;33(2):95-9.
-
Leonard MH. Trochanteric syndrome; calcareous and noncalcareous tendonitis and bursitis about the trochanter major. J. Am. Med. Assoc. 1958; 168:175Y7
-
Lequesne M, Mathieu P, Vuillemin-Bodaghi V, Bard H, Djian P. Gluteal tendinopathy in refractory greater trochanter pain syndrome: diagnostic value of two clinical tests. Arthritis Rheum. 2008;59:241-246.
-
Lindner D, Shohat N, Botser I, Agar G, Domb BG. Clinical presentation and imaging results of patients with symptomatic gluteus medius tears. Journal of Hip Preservation Surgery. 2015;2(3):310-315.
-
Long SS, Surrey DE, Nazarian LN. Sonography of greater trochanteric pain syndrome and the rarity of primary bursitis. AJR Am J Roentgenol. 2013;201:1083-1086.
-
Magnusson SP NM, Maganaris CN et al. Human tendon behaviour and adaptation, in vivo. J Physiol. 2008;30(1616-20).
-
Magnusson SP, Langberg H, Kjaer M. The pathogenesis of tendinopathy: balancing the response to loading. Nat Rev Rheumatol. 2010;6:262-268.
-
Mellor R, Grimaldi A, Wajswelner H, Hodges P, Abbott JH, Bennell K, Vicenzino B. Exercise and load modification versus corticosteroid injection versus ‘wait and see’ for persistent gluteus medius/minimus tendinopathy (the LEAP trial): a protocol for a randomised clinical trial. BMC Musculoskelet Disord. 2016 Apr 30;17:196.
-
Mulligan EP, Middleton EF, Brunette M. Evaluation and management of greater trochanter pain syndrome. Phys Ther Sport. 2015 Aug;16(3):205-14.
-
Noehren B, Scholz J, Davis I. The effect of real-time gait retraining on hip kinematics, pain and function in subjects with patellofemoral pain syndrome. Br J Sports Med. 2011;45(9):691–6.
-
Pfirrmann CW, Chung CB, Theumann NH, et al. Greater trochanter of the hip: attachment of the abductor mechanism and a complex of three bursae—MR imaging and MR bursography in cadavers and MR imaging in asymptomatic volunteers. Radiology. 2001;221(2): 469–77.
-
Pfirrmann CW, Notzli HP, Dora C, et al. Abductor tendons and muscles assessed at MR imaging after total hip arthroplasty in asymptomatic and symptomatic patients. Radiology. 2005;235(3):969–76.
-
Reid D. The management of greater trochanteric pain syndrome: A systematic literature review. Journal of Orthopaedics. 2016;13(1):15-28. doi:10.1016/j.jor.2015.12.006.
-
Robertson WJ, Gardner MJ, Barker JU, Boraiah S, Lorich DG, Kelly BT. Anatomy and dimensions of the gluteus medius tendon insertion. Arthroscopy. 2008;24:130-136.
-
Rompe JD et al. Home training, local corticosteroid injection, or radial shock wave therapy for greater trochanter pain syndrome. Am J Sports Med. 2009; 37(10):1981–90.
-
Sahrmann, SA. Diagnosis and treatment of movement impairment syndromes. Mosby, Inc; St. Louis, MO: 2002.
-
Schapira D, Nahir M, Scharf Y. Trochanteric bursitis: a common clinical problem. Arch Phys Med Rehabil. 1986 Nov;67(11):815-7.
-
Selkowitz DM, Beneck GJ, Powers CM. Which exercises target the gluteal muscles while minimizing activation of the tensor fascia lata? electromyographic assessment using fine-wire electrodes. J Orthop Sports Phys Ther. 2013; 43(2):54–64.
-
Shbeeb MI, Matteson EL. Trochanteric bursitis (greater trochanter pain syndrome). Mayo Clin Proc. 1996 Jun;71(6):565-9.
-
Sim FH, Scott SG. Injuries of the pelvis and hip in athletes: anatomy and function. In: Nicholas JA, Hershman EB, eds. The lower extremity and spine in sports medicine. St Louis, Mo: Mosby; 1986:1119-1169.
-
Stecco A, Gilliar W, Hill R, et al. The anatomical and functional relation between gluteus maximus and fascia lata. J Bodyw Mov Ther. 2013;17(4):512–7.
-
Stegemann H. Die chirurgische bedevtung paraartikularer kalkablagerungen. Arch. Klin. Chir. 1923; 125:718Y38.
-
Stern JR. Anatomical and functional specializations of the human gluteus maximus. Am J Phys Anthrop. 1972;36:315–40.
-
Strauss EJ, Nho SJ, Kelly BT. Greater trochanteric pain syndrome. Sports Med Arthrosc 2010;18: 113–119.
-
Sutter R, Kalberer F, Binkert CA, et al. Abductor tendon tears are associated with hypertrophy of the tensor fasciae latae muscle. Skel Radiol. 2013;42(5):627–33.
-
Thornton GM, Shao X, Chung M, et al. Changes in mechanical loading lead to tendon-specific alterations in MMP and tIMP expression: influence of stress deprivation and intermittent cyclic hydrostatic compression on rat supraspinatus and Achilles tendons. Br J Sports Med. 2010;44(10):698–703.
-
Vleeming A, Mooney V, Snijders C, et al. Movement, stability and low back pain: the essential role of the pelvis. New York: Churchill Livingstone; 1997.
-
Walsh G. MRI in greater trochanter pain syndrome. Australas Radiol. 2003;47(1):85–7.
-
Williams BS, Cohen SP. Greater trochanteric pain syndrome: a review of anatomy, diagnosis and treatment. Anesth Analg 2009;108:1662–70.
-
Williams RL, Warwick R. Gray’s Anatomy. 36th ed. Philadelphia, PA: Saunders; 1980.
-
Winston P, Awan R, Cassidy JD, et al. Clinical examination and ultrasound of self-reported snapping hip syndrome in elite ballet dancers. Am J Sports Med. 2007;35:118–126.
-
Woodley SJ, Mercer SR, Nicholson HD. Morphology of the bursae associated with the greater trochanter of the femur. J Bone Joint Surg Am 2008;90:284–94
-
Woodley SJ, Nicholson HD, Livingstone V, et al. Lateral hip pain: findings from magnetic 789 resonance imaging and clinical examination. J Orthop Sports Phys Ther. 2008;38:313-328.
-
Woyski D, Olinger A, Wright B. Smaller insertion area and inefficient mechanics of the 791 gluteus medius in females. Surg Radiol Anat. 2013;35:713-719.
-
Yen YM, Lewis CL, Kim YJ. Understanding and Treating the Snapping Hip. Sports Med Arthrosc. 2015 Dec;23(4):194-9.
-
Youdas JW, Foley BM, Kruger BL, et al. Electromyographic analysis of trunk and hip muscles during resisted lateral band walking. Physiother Theory Pract. 2013; 29(2):113–23.







